The most common adverse events reported with clarithromycin treatment include diarrhea, nausea, vomiting, abnormal taste, dyspepsia, abdominal pain/discomfort, rash and headache. Most of these effects were mild or moderate in severity.
Infections and infestations: Candidiasis, cellulitis, erysipelas, erythrasma, infection, pseudomembranous colitis, rhinitis, vaginal candidiasis, vaginal infection.
Blood and lymphatic system disorders: Anemia, agranulocytosis, eosinophilia, leukopenia, neutropenia, thrombocythemia, thrombocytopenia.
Immune system disorders: Anaphylactic reaction, anaphylactoid reaction, anaphylaxis, angioedema, hypersensitivity, myasthenia gravis.
Metabolism and nutrition disorders: Anorexia, decreased appetite, hypoglycemia.
Psychiatric disorders: Abnormal behavior, acute psychosis, anxiety, behavioral changes, confusion, confusional state, depersonalization, depression, disorientation, hallucination, insomnia, nervousness, mania/manic behavior, nightmare, psychotic behavior/disorder, psychosis, screaming.
Nervous system disorders: Abnormal dreams, ageusia, alteration of sense of smell, anosmia, convulsion, dizziness, dysgeusia, dyskinesia, loss of consciousness, nervousness, paresthesia, parosmia, somnolence, taste perversion, tremor.
Eye disorders: Conjuctivitis, corneal opacities, photophobia, visual disturbance.
Ear and labyrinth disorders: Deafness, ear disorder, hearing loss, hearing impaired, tinnitus, vertigo.
Cardiac disorders: Atrial fibrillation, cardiac arrest, electrocardiogram QT prolonged, extrasystoles, palpitations, torsades de pointes, ventricular arrhythmia/fibrillation/tachycardia.
Vascular disorders: Hemorrhage, vasodilation.
Respiratory, thoracic and mediastinal disorders: Asthma, cough, dyspnea, epistaxis, pharyngitis, pulmonary embolism.
Gastrointestinal disorders: Abdominal distention/pain, constipation, dark stools, dry mouth/thirst, eructation, esophagitis, flatulence, gastritis, gastroenteritis, gastrointestinal disorder, gastroesophageal reflux disease, glossitis, laryngiusmus, oral candidiasis/moniliasis, pancreatitis, proctalgia, rectal itching, stomatitis, tongue/tooth discoloration.
Hepatobiliary disorders: Cholestasis, jaundice (cholestatic and hepatocellular), hepatic failure, hepatic function abnormal, hepatitis, hepatitis cholestatic, hepatomegaly, liver function test abnormal.
Skin and subcutaneous tissue disorders: Acne, acute generalized exanthematous pustulosis, dermatitis, dermatitis bullous, diaper rash, drug rash with eosinophilia and systemic symptoms (DRESS), fixed drug eruption, Henoch-Schönlein purpura, hyperhidrosis, leukocytoclastic vasculitis, maculopapular rash, pruritus, purpuric rash, severe cutaneous adverse reactions (SCAR), Stevens-Johnson syndrome, toxic epidermal necrosis, urticaria.
Musculoskeletal and connective tissue disorder: Back pain, muscle spasms, musculoskeletal stiffness, myalgia, myopathy, nuchal rigidity, rhabdomyolysis.
Renal and urinary disorders: Hematuria, interstitial nephritis, renal failure.
Reproductive system and breast disorders: Dysmenorrhea.
General disorders and administration site conditions: Asthenia, chest pain, chills, fatigue, influenza, malaise, pain, pyrexia.
Investigations: Alanine aminotransferase increased, albumin globulin ratio abnormal, amylase increased, aspartate aminotransferase increased, blood alkaline phosphatase increased, blood alkaline phosphatase increased, blood lactate dehydrogenase increased, blood bilirubin increased, blood creatinine increased, blood urea increased, gamma-glutamyltransferase increased, hemoglobin decreased, international normalized ratio (INR) increased, liver enzymes increased, liver function test abnormal, platelet count decreased, prothrombin time prolonged, urine color abnormal, white blood cell count decreased.
Clinical Trials Experience: All-Cause Mortality in Patients with Coronary Artery Disease 1 to 10 Years Following Clarithromycin Exposure: In one clinical trial evaluating treatment with clarithromycin on outcomes in patients with coronary artery disease, an increase in risk of all-cause mortality was observed in patients randomized to clarithromycin. Clarithromycin for treatment of coronary artery disease is not an approved indication. Patients were treated with clarithromycin or placebo for 14 days and observed for primary outcome events (e.g., all-cause mortality or non-fatal cardiac events) for several years. A numerically higher number of primary outcome events in patients randomized to receive clarithromycin was observed with a hazard ratio of 1.06 (95% confidence interval 0.98 to 1.14). However, at follow-up 10 years post-treatment, there were 866 (40%) deaths in the clarithromycin group and 815 (37%) deaths in the placebo group that represented a hazard ratio for all-cause mortality of 1.10 (95% confidence interval 1.00 to 1.21). The difference in the number of deaths emerged after one year or more after the end of treatment. The cause of the difference in all-cause mortality has not been established. Other epidemiologic studies evaluating this risk have shown variable results (see Precautions).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image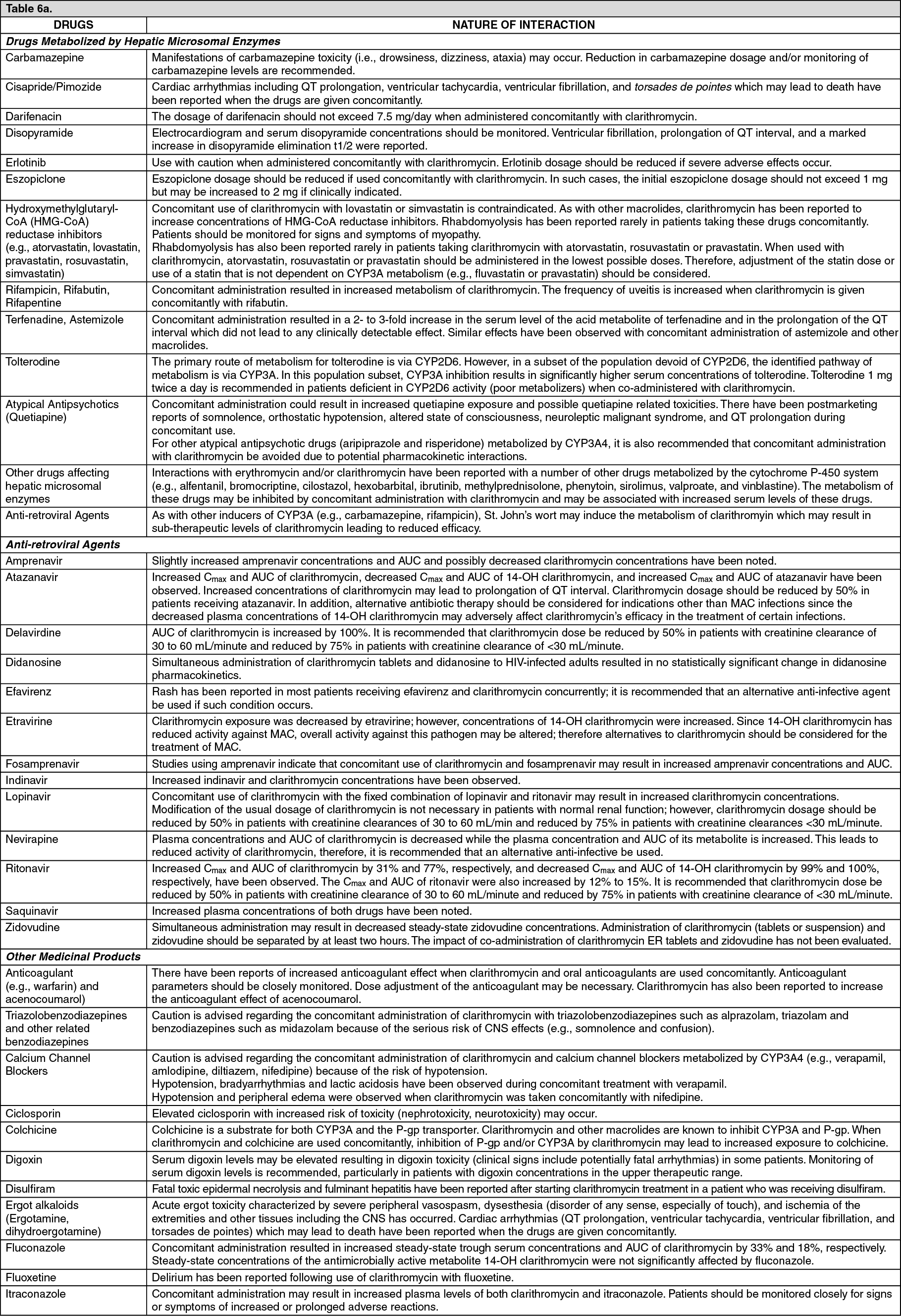 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image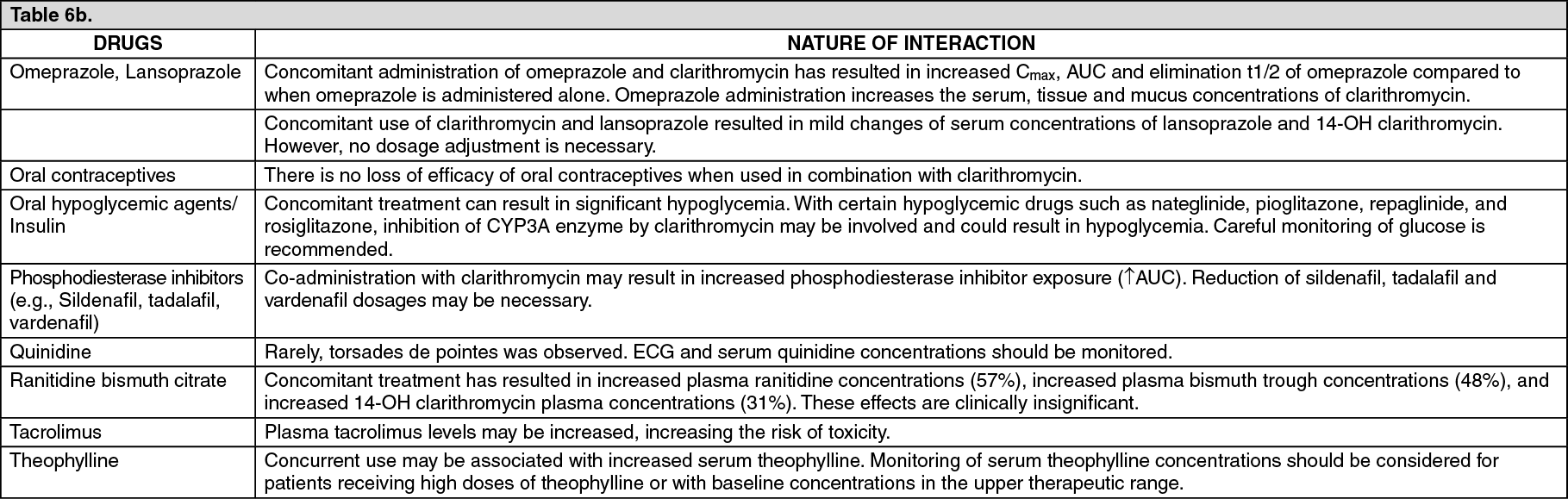 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
